Scientific classification
Kingdom: Chromalveolate
superphylum : Alveolata
phylum : Apicomplexa
class : Aconoidasida
order : Haemosporodia
family : Plasmodiidae
genus: Plasmodium
===================
Malaria is caused by protozoa of the Plasmodium species.
There are more than 200 known species of plasmodium but only five species , known till now, infect both humans and animals :
Plasmodium malariae (quartian malaria)
Plasmodium vivax (benign tertian malaria)
Plasmodium falciparum (malignant tertian malaria, subtertian malaria)
Plasmodium ovale (ovale tertian malaria).
Plasmodium knowlesi
Life cycle :
The transmission of Plasmodium requires two hosts, an intermediate invertebrate host (vector), and a definitive vertebrate host (mammals, birds and lizards).
All Plasmodium species undergo the general haemosporina developmental cycle which can be summarized as:
- initial or continual schizogony (reproduction by multiple asexual fission) in the vertebrate host with initiation of gametogony (the formation or production of gametes);
- formation of gametes in the arthropod host and subsequent fertilization and formation of a zygote
- formation of sporozoites from the zygote by repeated nuclear division followed by cytoplasmic divisions.
Malaria is transmitted by the female anopheline mosquito
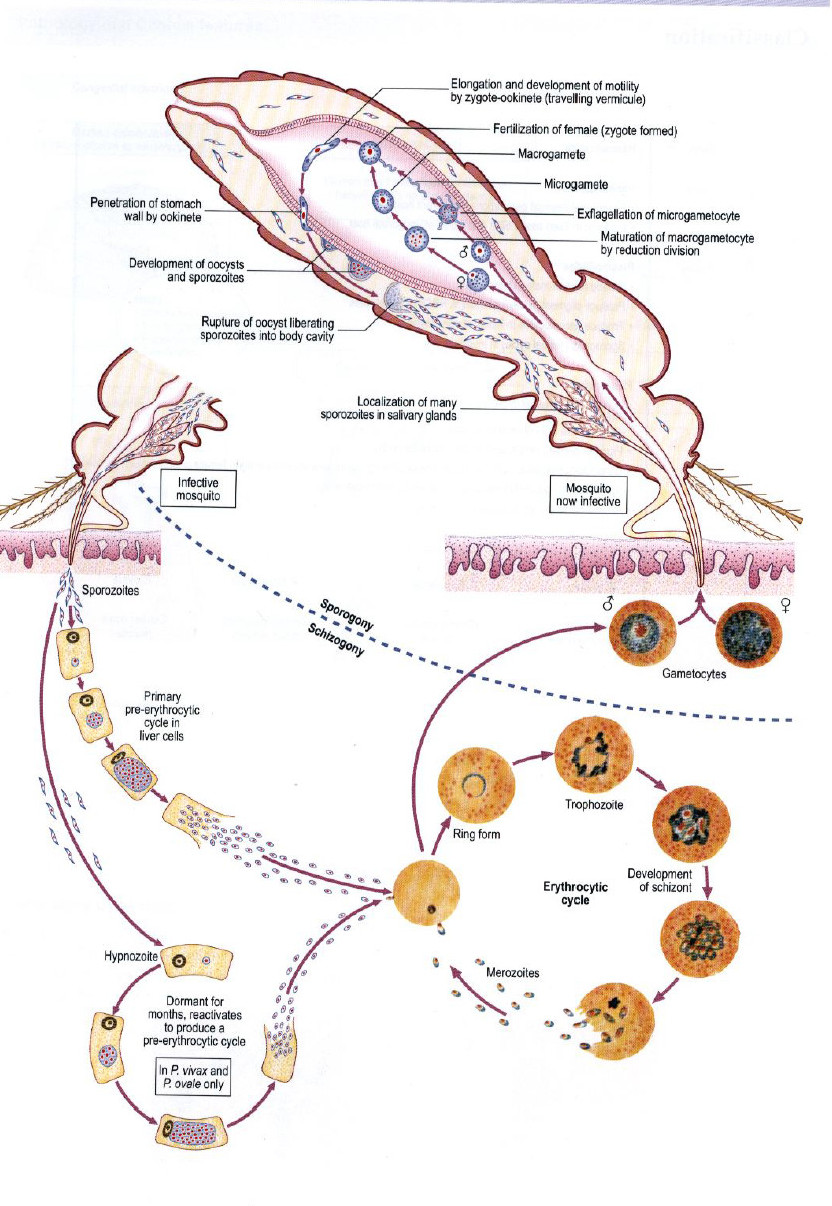
The life cycle of all species of human malaria parasites is essentially the same.
It comprises an exogenous sexual phase (sporogony) with multiplication in certain Anopheles mosquitoes and an endogenous asexual phase (schizogony) with multiplication in the vertebrate host.
The latter phase includes the development cycle in the red cells (erythrocytic schizogony) and the phase taking place in the parenchyma cells in the liver (pre-erythrocytic schizogony).
When a female Anopheles mosquito bites an infected person, it ingests blood which may
contain the mature sexual cells (male and female gametocytes) which undergo a series of
developmental stages in the stomach of the mosquito.
Exflagellation (the extrusion of rapidlywaving flagellum-like microgametes from microgametocytes) occurs resulting in the production in a number of male and female gametes.
Fertilization occurs producing a zygote which maturesto an ookinete. This penetrates the stomach wall of the mosquito where it grows into an oocyst and it further matures to become a motile sporozoite.
The length of the developmental stage in the mosquito not only depends on the Plasmodium
species but also the mosquito host and the ambient temperature.
This may range from eight days in Plasmodium vivax to as long as 30 days in Plasmodium malariae
The sporozoites migrate from the body cavity of the mosquito to the salivary glands and the
mosquito now becomes infective.
Sporozoites enter into the blood stream of a host when the mosquito feeds on blood.
Following the inoculation, the sporozoites leave the blood within 40 minutes and enter the parenchymal cells of the liver .
In all five species, asexual development occurs in the liver cells, a process produce thousands of tiny merozoites which are released into the circulation after about 16 days.
However in P. vivax and P. ovale ( only ) some sporozoites differentiate into hypnozoites which remain dormant in hepatocytes for considerable periods of time. When they are “reactivated” they undergo asexual division and produce a clinical relapse.
Once in the circulation, the merozoites invade the red cells and develop into trophozoites.
In the course of their development they absorb the hemoglobin of the red cells and leave as the product of digestion a pigment called hemozoin, a combination of hematin and protein. Thisiron-containing pigment is seen in the body of the parasite in the form of dark granules, which are more obvious in the later stages of development.
After a period of growth the trophozoite undergoes an asexual division, erythrocytic schizogony. When the mature trophozoite starts to divide in the red blood cell, separate merozoites are formed resulting in a schizont. When fully developed, the schizont ruptures the red blood cell containing it, liberating the merozoites into the circulation. These merozoites will then infect new red cells and the process of asexual reproduction in the blood tends to proceed.
Some of the merozoites entering red blood cells do not form trophozoites then schizonts but
develop into gametocytes and this process takes place in deep tissue capillaries. This
erythrocytic cycle of schizogony is repeated over and over again in the course of infection,
leading to a progressive increase of parasitemia.

female Anopheles the vector of the protozoa group Plasmodia
plasmodium life-cycle
Clinical features :
Infections with all four strains of malaria have many clinical features in common.
These are related to the liberation of fever-producing substances, especially during schizogony.
Fever: Often irregular. The regular pattern of fever does not occur until the illness has
continued for a week or more; where it depends on synchronized schizogony.
Anemia: The anemia is hemolytic in type. It is more severe in infections with P. falciparum because in this infection cells of all ages can be invaded. Also, the parasitemia in this infection can be much higher than in other malarias.
Splenomegaly: The spleen enlarges early in the acute attack of malaria. When a patient has been subjected to many attacks, the spleen may be of an enormous size and lead to secondary hypersplenism.
Jaundice: A mild jaundice due to hemolysis may occur in malaria. Severe jaundice only
occurs in P. falciparum infection, and is due to liver involvement.

Clinical features
Diagnosis :
- microscopical examination of thin and thick blood films for malaria parasites and for species determination using Giemsa and Field’s stain.
- parasitaemia estimation to indicate severity of infection and effectiveness of treatment.
- immunochromatographic techniques for the detection of malaria antigen in blood.
- PCR for malaria confirmation and species determination when required.
Notes :
It is important to report the level of parasitemia when blood films are examined and found to be positive for malaria parasites Because of the potential for drug resistance in some of the Plasmodium species, particularly Plasmodium falciparum.
This allows the parasitemia to be monitored after therapy has been initiated. In cases where the patient is hospitalized, monitoring should be performed at 24, 48, and 72 h after initiating therapy. Generally the parasitemia will drop very quickly within the first 2 h; however, in cases of drug resistance, the level may not decrease but actually increase over time.
The specimen consists of stained thick or thin blood films that have been examined a minimum of 300 oil immersion fields per blood film to determine that the film is positive for malaria parasites.
malaria parasites may be missed on a thin blood film when there is a low parasitemia. Therefore, examination of a thick blood film is recommended. With a thick blood film, the red cells are approximately 6-20 layers thick which results in a larger volume of blood being examined.
A. Thin blood film: counting several hundred to 1,000 RBCs, report the percentage of infected RBCs per 100 RBCs counted (0.5%, 1.0%, etc.).
B. Thick or thin blood film: counting 100 WBCs (or more), report the number of parasites per 100 WBCs on the smear.
1. This figure can be converted to the number of parasites per microliter of blood; divide the number of parasites per 100 WBCs by 100, and multiply that figure by the number of WBCs per microliter of blood.
2. Depending on the parasitemia, 200 or more WBCs may have to be counted, so the denominator may vary (it may be 200 or even more).
3. Using this method, blood for both the peripheral smears and cell counts must be collected at the same time.
LIMITATIONS OF THE PROCEDURE :
A. A light infection may be missed in a thin film, whereas the increased volume of blood present on a thick film may allow the detection of the infection, even with a low parasitemia.
B. If the smears are prepared from anticoagulated blood that is more than 1 h old, the morphology of both parasites and infected RBCs may not be typical Where the following effects may be seen.
1. Sexual stages may continue to develop and male gametocytes can exflagellate, liberating gametes into the plasma. These can be mistaken for organisms such as Borrelia.
Gametocytes of P. falciparum which have a characteristic crescent shape, may round up and then resemble those of P. malariae.
2. Accole forms, which are characteristic of P. falciparum, may be seen in P. vivax because of attempted re – invasion of the red blood cell by merozoites.
3. Mature trophozoites of P. vivax may condense when exposure becomes prolonged and in cases of extreme exposure, red blood cells containing gametocytes and mature schizonts may be totally destroyed along with the contained parasites. The malaria pigment, hemozoin, always remains and can provide a clue to the presence and, to an expert eye.
4. The morphology of the red blood cell may be altered by shrinkage or crenation.

Preparation of thick and thin blood smear
Treatment
Treatment varies greatly depending on the species, drug resistance and severity of the infection.
Drugs include: Chloroquine, Sulfadoxine-pyrimethamine, Quinine, Primaquine
Treatment should be continued until the elimination of the parasites is confirmed.